
Reviewed by Dr. Shradha Chakhaiyar, MBBS, DGO, MRCOG (London), IVF Specialist & Reproductive Surgeon
Shradha IVF & Maternity, Patna, Bihar · 20+ Years Clinical Experience
📋 Table of Contents
- What Is Low Ovarian Reserve?
- Signs and Symptoms
- What Causes It? — 7 Known Causes
- How Is It Diagnosed? (AMH, AFC, FSH)
- AMH Levels by Age — Reference Table
- Can You Get Pregnant With Low Reserve?
- Treatment Options — Full Guide
- IVF Success Rates by Age
- Diet & Lifestyle — The 3-Month Window
- When to See a Fertility Specialist
- Treatment at Shradha IVF, Patna
- Frequently Asked Questions
What Is Low Ovarian Reserve?
Low ovarian reserve — also called diminished ovarian reserve (DOR), or low egg count, or poor ovarian reserve, or decreased ovarian reserve. It is a condition in which a woman has fewer eggs in her ovaries than expected for her age. It is most commonly diagnosed when AMH (Anti-Müllerian Hormone) is below 1.0 ng/mL, antral follicle count on ultrasound is below 5–7, or day-3 FSH is above 10–15 mIU/mL. Low ovarian reserve makes natural conception more difficult and may shorten the reproductive timeline, but it does not mean infertility. With proper diagnosis and treatment, pregnancy remains possible.
The word “reserve” can be misleading. It does not mean a savings account of eggs that you can dip into when ready — it means the pool of eggs remaining in your ovaries at any given moment. Every woman is born with all the eggs she will ever have. The ovaries do not produce new eggs after birth. From the moment of birth, the egg pool only decreases — never replenishes.
What “low ovarian reserve” tells us is that your remaining pool is smaller than typical for your age. It does not tell us about the quality of the remaining eggs. It does not tell us whether you can conceive naturally — many women with low AMH conceive naturally. What it does tell us is how your ovaries are likely to respond to fertility stimulation: how many eggs we can expect to retrieve in an IVF cycle, and how soon your reproductive window may close.
The Egg Count Timeline — From Birth to Menopause
Understanding low ovarian reserve starts with understanding that every woman’s egg count follows the same predictable curve:
- Before birth (5th month of pregnancy): 6–7 million eggs — the lifetime peak
- At birth: 1–2 million eggs — already declining
- At puberty (~age 12): 300,000–400,000 eggs — only about 400 will ever ovulate
- At age 30: 100,000–150,000 eggs
- At age 35: 50,000–80,000 eggs — the decline accelerates from this point
- At age 40: approximately 25,000 eggs — quality drops sharply alongside quantity
- At menopause (~age 51): fewer than 1,000 eggs remaining — functional reserve depleted
The most important number on this timeline is age 35 — the point at which the rate of decline shifts from gradual to steep. This is why most fertility guidelines recommend evaluation by age 35 if you have been trying to conceive, and why low AMH at any age before 35 deserves immediate clinical attention rather than a “wait and see” approach.
3 monthsFor egg quality changes to take effect
What are the Signs and Symptoms of Decreased/Low Ovarian Reserve?
The most important thing to know about low ovarian reserve is that most women have no symptoms at all. The condition is usually discovered during fertility testing, not because of any warning sign. This is why women who are not actively trying to conceive often only learn they have low AMH after months — or years — of unsuccessful attempts at pregnancy.
When symptoms do appear, they include:
- Difficulty conceiving — typically after 12 or more months of regular unprotected intercourse in women under 35, or after 6 months in women over 35
- Shorter menstrual cycles — cycles shortening from a normal 28 days to 25–26 days, sometimes the earliest measurable sign
- Irregular menstrual periods — periods of less duration or irregular periods is more common in PCOS than DOR
- Symptoms of primary ovarian insufficiency (POI) — if low reserve is severe and occurs before age 40, women may experience hot flushes, night sweats, vaginal dryness, and mood changes typically associated with perimenopause
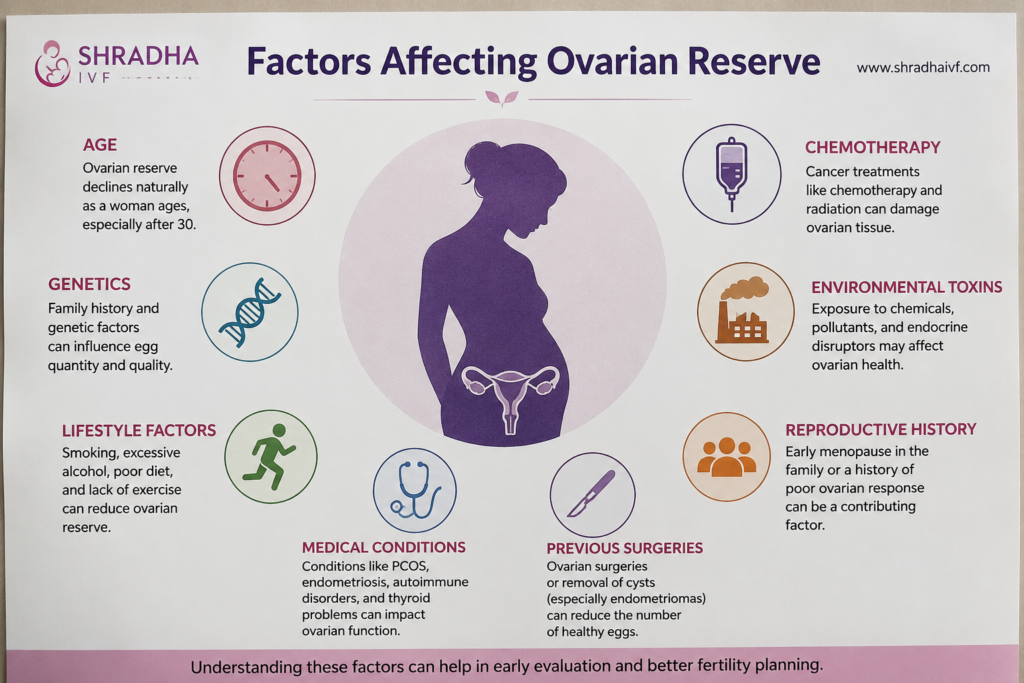
What Causes Low Ovarian Reserve? — 7 Known Causes
Age is by far the most common cause of low ovarian reserve — the egg pool naturally diminishes over time, and the rate of decline varies between women based on genetics. However, several other factors can accelerate this process or cause low ovarian reserve at a younger-than-expected age:
- Age — the dominant cause. Ovarian reserve declines from birth, accelerates after age 35, and drops steeply after age 40. This is normal physiology, not a disease.
- Smoking and tobacco use. According to the American Society for Reproductive Medicine, smoking is the only lifestyle factor with strong scientific evidence linking it directly to reduced ovarian reserve. This includes smoking and smokeless tobacco use, which is significant in parts of Bihar.
- Genetic conditions affecting the X chromosome. Fragile X premutation, Turner syndrome variants, and certain BRCA gene mutations are associated with earlier-than-expected ovarian decline.
- Cancer treatments. Chemotherapy and pelvic radiation can damage ovarian tissue and accelerate egg loss. The effect depends on the specific drug, dose, and age at treatment.
- Ovarian surgery. Removal of one or both ovaries (oophorectomy), surgical treatment of ovarian endometriomas, or large ovarian cyst removal can directly reduce the egg pool.
- Endometriosis. Chronic inflammation from endometriosis — particularly ovarian endometriomas (chocolate cysts) — has been shown to accelerate AMH decline. This is one of the most under-recognised contributors to early-onset low ovarian reserve.
- Autoimmune conditions. Systemic lupus erythematosus, certain thyroid disorders, and other autoimmune diseases can cause autoimmune damage to ovarian tissue.
In approximately 30% of cases, no identifiable cause is found. This is called idiopathic low ovarian reserve, and it does not mean the diagnosis is wrong — it simply means we cannot pinpoint why a particular woman’s egg pool is lower than expected. Importantly, two factors that many patients ask about are not known causes of low ovarian reserve:
- Stress — there is no scientific evidence that psychological stress causes low ovarian reserve, although managing stress is still important for overall fertility outcomes
- Oral contraceptive use — birth control pills may suppress AMH temporarily but do not deplete the underlying egg pool
How Is Low Ovarian Reserve Diagnosed? — AMH, AFC, FSH and Estradiol
Low ovarian reserve cannot be diagnosed from one test alone. The standard evaluation combines a blood test (AMH) with an ultrasound (antral follicle count) and, often, additional day-3 hormone tests. Each test measures a different aspect of ovarian function, and they are interpreted together.
The AMH Test — What Your Numbers Mean by Age
Anti-Müllerian Hormone (AMH) is a protein produced by the small follicles in the ovaries. The amount of AMH in your blood reflects the size of your remaining follicle pool. AMH can be tested on any day of the menstrual cycle — it does not fluctuate substantially through the month, unlike FSH or estradiol — making it the most convenient and reliable single marker of ovarian reserve.
AMH levels naturally decline with age, so “normal” must always be interpreted in the context of your age:
| Age Range | Typical AMH (ng/mL) | Low / DOR Range | Clinical Note |
|---|---|---|---|
| Under 25 | 3.0 – 5.0+ | < 1.5 | Peak fertility window |
| 25 – 29 | 2.5 – 4.5 | < 1.5 | AMH typically peaks around 25 |
| 30 – 34 | 1.8 – 3.5 | < 1.2 | Gradual decline begins |
| 35 – 37 | 1.2 – 2.5 | < 1.0 | Decline accelerates |
| 38 – 40 | 0.8 – 1.8 | < 0.7 | Fertility drops sharply |
| 41 – 42 | 0.5 – 1.2 | < 0.4 | Severely diminished |
| Over 42 | < 0.5 | < 0.2 | Donor egg discussion warranted |
The widely-used POSEIDON criteria define an AMH of less than 1.2 ng/mL as the threshold for “poor ovarian response” in IVF — meaning the ovaries are unlikely to produce many eggs in a standard stimulation cycle. The Cleveland Clinic defines AMH below 1.0 ng/mL as low and below 0.4 ng/mL as severely low. Different laboratories use slightly different reference ranges, so always interpret your result against the lab’s own cutoffs and discuss it with your fertility specialist.
Antral Follicle Count (AFC) — The Ultrasound Test
The antral follicle count is performed during a transvaginal ultrasound, usually between Day 2 and Day 5 of your menstrual cycle. The sonographer counts the small follicles (2–10 mm in diameter) visible in both ovaries. This number correlates closely with the AMH result and gives a real-time picture of how the ovaries are likely to respond to stimulation.
| AFC (Both Ovaries) | Ovarian Reserve Status | Expected IVF Response |
|---|---|---|
| More than 15 | High (possible PCOS) | High responder — risk of OHSS, protocol adjustment |
| 8 – 15 | Normal | Standard IVF protocol |
| 5 – 7 | Borderline low | Mild stimulation or antagonist protocol |
| Less than 5 | Low / DOR | Mini-IVF, multiple-cycle banking, or donor consideration |
FSH and Estradiol — The Day-3 Hormones
Day-3 FSH (follicle-stimulating hormone) and estradiol are measured on day 2 or 3 of your menstrual cycle. In women with normal ovarian reserve, FSH is typically below 10 mIU/mL on day 3. As ovarian reserve declines, the pituitary gland produces more FSH in an attempt to stimulate the ovaries, so an elevated FSH (above 10–15 mIU/mL) suggests diminished reserve. Estradiol is measured at the same time because high estradiol can artificially suppress FSH and mask the true picture.
Can You Get Pregnant With Low Ovarian Reserve?
Yes — pregnancy is possible with low ovarian reserve, both naturally and with fertility treatment. The single most important fact about low ovarian reserve is that it only takes one healthy egg and one healthy sperm to create a pregnancy.
Research from the Centre for Reproductive Health has reported that approximately 33% of women with diminished ovarian reserve achieve pregnancy with their own eggs after appropriate fertility treatment. Egg quantity is one factor in fertility, but so is egg quality, sperm quality, fallopian tube patency, uterine receptivity, and timing. A low number on a test does not eliminate any of these other factors from your favour.
However, low ovarian reserve does shorten your window for pregnancy with your own eggs. The clinical strategy is therefore not to wait — it is to evaluate sooner, plan treatment if needed, and consider fertility preservation early if you are not yet ready to conceive.
What are the Treatment Options for Low Ovarian Reserve
There is no medical treatment that increases the number of eggs in your ovaries — biology does not allow it. What we can do is maximise the chance of pregnancy using the eggs that remain. The right treatment depends on your age, your AMH level, your partner’s sperm parameters, how urgently you want to conceive, and how many cycles you are willing to undertake.
Lifestyle Changes That Support Egg Quality
You cannot grow new eggs, but you can support the quality of the eggs you have. The 90-day window before ovulation is when an egg is most sensitive to its environment — this is why all lifestyle interventions take approximately three months to show effect.
- Stop smoking and tobacco use — the only lifestyle factor with strong evidence for direct ovarian reserve damage
- Reach a healthy weight — both underweight and obesity affect hormone balance and egg quality
- Adopt a Mediterranean-style diet — high in vegetables, fruits, whole grains, olive oil, nuts, legumes, and fish; lower in red meat and refined sugar
- Manage thyroid function and vitamin D — both are commonly deficient in Indian women, and both affect ovarian function
- Sleep 7–8 hours per night and reduce chronic stress — supportive of overall reproductive function
- Limit alcohol — heavy drinking is associated with poorer fertility outcomes
- Moderate exercise — regular movement is beneficial; extreme endurance training is not
Supplements — CoQ10, DHEA, Vitamin D, Omega-3
- Coenzyme Q10 (CoQ10): Antioxidant that supports mitochondrial function in eggs. Most-studied supplement for egg quality. Typical dose in research: 200–600 mg daily for at least 90 days before egg retrieval.
- DHEA (Dehydroepiandrosterone): Mild androgen used in some DOR protocols. Some studies report improved IVF outcomes and reduced miscarriage rates. Typical dose: 25 mg three times daily, but only under medical supervision.
- Vitamin D: Many Indian women are vitamin D deficient. Low vitamin D is associated with lower AMH. Correcting deficiency is supportive of ovarian function.
- Omega-3 fatty acids: Anti-inflammatory effects and possible direct support of egg quality.
- Folate (methylfolate preferred): Essential for egg development and early embryo health.
- Inositol: Particularly useful in women with co-existing PCOS; supports insulin sensitivity and ovarian function.
IUI With Mild Stimulation
A 2025 pilot study comparing strategies in women under 40 with diminished ovarian reserve found that beginning with intrauterine insemination (IUI) plus mild ovarian stimulation, before progressing to IVF, may produce higher cumulative clinical pregnancy rates than starting directly with IVF. IUI with mild stimulation is less expensive than IVF, less physically demanding, and appropriate as a first-line option for many younger women with DOR who have at least one open fallopian tube and normal sperm parameters.
IVF — Standard and Mini-IVF Protocols
For women with low ovarian reserve, IVF is the most effective single treatment. The protocol choice matters significantly:
- Antagonist protocol — most commonly used for DOR; shorter duration, more flexibility, lower medication burden
- Mini-IVF or mild stimulation — uses lower medication doses, retrieves fewer but often higher-quality eggs, reduces cost and side effects, suitable for poor responders
- Multiple-cycle banking — collecting eggs or embryos across 2–3 cycles before transfer, building a usable cohort
- DuoStim protocol — stimulating twice in the same menstrual cycle to maximise eggs retrieved
Egg or Embryo Freezing
If you have been diagnosed with low ovarian reserve and are not yet ready to attempt pregnancy, fertility preservation is a serious option to discuss. Egg freezing retrieves and stores unfertilised eggs for future use. Embryo freezing fertilises retrieved eggs with partner or donor sperm and stores the embryos. Embryos generally survive freezing and thawing better than eggs, but freezing eggs preserves more future flexibility. Both procedures decrease in success rate as the woman ages, so earlier action produces better outcomes.
Donor Eggs — and the Indian Legal Framework
When ovarian reserve is severely diminished or repeated IVF cycles with own eggs have failed, donor egg IVF offers consistently high success rates — typically 50–60% per transfer cycle, regardless of the recipient’s age. In India, egg donation is regulated under the Assisted Reproductive Technology (Regulation) Act, 2021. Donation is anonymous, donors are medically screened, and the resulting child is legally the recipient couple’s child. The donor’s egg is fertilised with your partner’s sperm, creating an embryo that carries your partner’s genetic material — and you carry and give birth to the baby.
IVF Success Rates With Low Ovarian Reserve — by Age
Honesty about success rates is essential. Age affects IVF outcomes more strongly than AMH alone. The following are typical per-cycle live birth rates for women with diminished ovarian reserve at various ages:
| Age Bracket | Own Eggs (per cycle) | Own Eggs (cumulative, 3 cycles) | Donor Eggs (per cycle) |
|---|---|---|---|
| Under 35 | 35 – 45% | 60 – 70% | 50 – 60% |
| 35 – 37 | 25 – 35% | 45 – 55% | 50 – 60% |
| 38 – 40 | 15 – 25% | 30 – 40% | 50 – 60% |
| 41 – 42 | 8 – 12% | 20 – 30% | 50 – 60% |
| Over 42 | 3 – 6% | 10 – 15% | 50 – 55% |
Two things stand out from this data. First, cumulative success across multiple cycles is meaningfully higher than per-cycle success — meaning a woman who is willing to undertake more than one cycle has substantially better odds than her first-cycle number alone suggests. Second, donor egg cycles maintain consistent success regardless of the recipient’s age — because the limiting factor in IVF outcome at older ages is egg quality, not uterine receptivity.
Diet & Lifestyle for Improving Egg Quality — The 3-Month Window
One of the most useful and least-explained facts about fertility biology: the eggs that ovulate in any given month were “recruited” approximately 90 days earlier. During those three months, the egg is highly sensitive to its environment — to your nutrition, sleep, stress levels, blood sugar, and exposure to toxins. This means that lifestyle interventions take time to show effect, and that beginning preparation three months before a planned IVF cycle is clinically meaningful.
Foods that consistently appear in the egg-quality-supporting evidence include:
- Leafy green vegetables — spinach, methi, sarson — are rich in folate
- Berries and citrus fruits — high in antioxidants
- Nuts and seeds — almonds, walnuts, flax, chia — for omega-3 and protein
- Fatty fish or omega-3 supplementation if fish is not in the diet
- Whole grains and legumes — for stable blood sugar
- Olive oil and avocado — for monounsaturated fats
- Eggs and lean protein — for choline and amino acids that support egg development
What to limit: highly processed foods, sugar-sweetened beverages, trans fats, excessive caffeine (more than 200 mg daily is associated with reduced fertility), alcohol, and any tobacco product.
When Should You See a Fertility Specialist for Decreased Ovarian Reserve?
Most women do not need to see a fertility specialist as a first step. But certain situations warrant earlier evaluation rather than waiting:
- Under 35 and trying for 12 months with no pregnancy
- Aged 35 to 39 and trying for 6 months with no pregnancy
- Aged 40 or above — see a specialist immediately when planning pregnancy, regardless of how long you have been trying
- Family history of early menopause — proactive evaluation in your early thirties
- Known endometriosis, PCOS, or thyroid disorder — earlier evaluation regardless of age
- Prior ovarian surgery, chemotherapy, or pelvic radiation — discuss reserve testing
- Irregular or shortened menstrual cycles at any age
Poor Ovarian Reserve Treatment at Shradha IVF in Patna
At Shradha IVF, every patient with low ovarian reserve receives a complete baseline evaluation — AMH, AFC, day-3 hormones, partner semen analysis, thyroid and vitamin D screening, and a uterine cavity assessment — before any treatment is started. We do not recommend rushed cycles. We do not push donor eggs as a first option for women who still have their own-egg potential. We are transparent about expected outcomes and about cost.
- Personalised IVF protocols: antagonist, mini-IVF, multiple-cycle banking — protocol selected based on your AMH, AFC, and age, not a one-size template
- Free pre-treatment consultation: available at our regular IVF Camp
- IVF Cost Calculator: get a transparent estimate before booking
- EMI options: IVF on EMI for couples who need financial flexibility
- Direct guidance from Dr. Shradha Chakhaiyar — every patient’s treatment plan is reviewed and signed off personally, not delegated
FAQs on Decreased Ovarian Reserve
Low ovarian reserve means the number and sometimes the quality of eggs in the ovaries are lower than expected for a woman’s age. This can make it more difficult to conceive naturally because fewer healthy eggs are available for ovulation and fertilization. Women with low ovarian reserve may experience irregular periods, poor response to fertility medications, or difficulty getting pregnant, although some women may still have regular cycles and no obvious symptoms.
Treatment for diminished ovarian reserve depends on age, fertility goals, and overall reproductive health. Doctors may recommend lifestyle improvements, fertility medications, ovarian stimulation, IVF, egg freezing, or donor eggs in some cases. Early fertility evaluation and timely treatment are important because ovarian reserve naturally declines with age.
Healthy blood circulation supports ovarian function and reproductive health. Doctors may suggest lifestyle changes such as regular exercise, stress management, proper sleep, hydration, and a balanced diet rich in antioxidants. Some fertility specialists may also recommend supplements, yoga, or therapies that support pelvic circulation, although treatment should always be personalized based on medical advice.
Yes, IVF can be an effective treatment option for women with low ovarian reserve, especially when natural conception becomes difficult. IVF helps by stimulating the ovaries to retrieve available eggs for fertilization. However, success rates depend on factors such as age, egg quality, hormone levels, and overall fertility health. Early treatment often improves outcomes.
Yes, it is still possible to conceive with low ovarian reserve. Many women achieve natural pregnancy or successful IVF pregnancies despite reduced egg reserve. The chances depend on factors like age, egg quality, ovulation, and overall reproductive health. Consulting a fertility specialist early can help identify the best treatment options and improve pregnancy chances.
Your Poor Ovarian Reserve Is Not Your Destiny.
One blood test does not decide your fertility. At Shradha IVF & Maternity in Patna, Dr. Shradha Chakhaiyar reads your numbers alongside your full clinical picture — and builds a treatment plan that is honest, personalised, and respectful of every part of your journey.
Book Your Free Consultation →