
Reviewed by Dr. Shradha Chakhaiyar, MBBS, DGO, MRCOG (London), IVF Specialist & Reproductive Surgeon
Shradha IVF & Maternity, Patna, Bihar · 20+ Years Clinical Experience
📋 Table of Contents
- What Is a Blastocyst?
- Why Day-5 Embryos Succeed — 3 Reasons
- Day 3 vs Day 5 — The Honest Comparison
- Decoding Your Embryo Grade (4AA, 3BB)
- Day 5 vs Day 6 Blastocyst
- Who Should — and Shouldn’t — Choose It
- Blastocyst, PGT-A & Single Embryo Transfer
- Cost & Lab Capability in India
- Blastocyst Transfer at Shradha IVF
- Frequently Asked Questions
What Is a Blastocyst? — Day 3 vs Day 5 Embryo Development
A blastocyst is an embryo that has developed for 5 to 6 days after fertilisation, reaching an advanced stage with around 100–200 cells organised into distinct parts: the inner cell mass (which becomes the baby) and the trophectoderm (which becomes the placenta), surrounding a fluid-filled cavity. Blastocyst transfer means placing this Day-5 embryo into the uterus instead of an earlier Day-3 embryo. Because blastocysts are more developed and naturally synchronised with the uterus, they typically have a higher implantation rate per embryo transferred.
To understand blastocyst transfer, it helps to follow what happens to an embryo in the days after fertilisation:
- Day 1: The egg is fertilised by sperm, forming a single cell (the zygote).
- Day 2–3: The embryo divides into a “cleavage-stage” embryo — a small ball of 6 to 8 cells called blastomeres. At this stage, the embryo is still running mostly on instructions inherited from the egg.
- Day 4: The cells compact together into a structure called a morula.
- Day 5–6: A fluid-filled cavity forms and the embryo organises itself into a blastocyst — with two clearly different cell types: the inner cell mass (the cluster that becomes the foetus) and the trophectoderm (the outer layer that becomes the placenta).
So the choice in IVF is essentially this: transfer the embryo earlier, at the Day-3 cleavage stage, or wait and transfer it at the Day-5 blastocyst stage. Both are valid. But there are real biological reasons why Day-5 transfer often improves the odds — and equally real reasons why it isn’t right for everyone.
Day 5When an embryo naturally reaches the uterus
Why Do Day-5 Embryos Have Higher IVF Success? — The Three Reasons
Day-5 blastocyst transfer improves the odds of implantation for three reasons. Understanding them is the key to understanding the whole topic.
1. Natural Synchrony With the Uterus
This is the most intuitive reason. In a natural pregnancy, the embryo does not arrive in the uterus immediately. After fertilisation in the fallopian tube, it travels down over several days, only reaching the uterine cavity at around Day 5 — exactly when it has become a blastocyst. A Day-3 embryo transferred into the uterus is, in a sense, arriving “early” compared to nature. A Day-5 blastocyst transfer places the embryo into the uterus at precisely the stage and time nature intended — when the uterine lining is most receptive, and the embryo is biologically ready to implant. This synchrony is a genuine physiological advantage.
2. Natural Selection of Stronger Embryos
This is the most powerful reason — and the one that most directly answers the question every patient is really asking: “Will this embryo actually become a baby?” Many embryos that look perfectly normal on Day 3 carry chromosomal abnormalities that prevent them from developing further. These weaker embryos frequently arrest — stop growing — between Day 3 and Day 5. So by culturing embryos to Day 5, the laboratory lets nature perform a screening step: the embryos that survive to the blastocyst stage are, on average, more likely to be chromosomally normal and genuinely viable. You are no longer guessing which Day-3 embryo is best — you are transferring one that has already proven its developmental strength.
3. Better Embryo Selection by the Embryologist
A Day-3 embryo offers limited information — the embryologist can count cells and assess fragmentation, but morphology on Day 3 has limited power to predict what happens next. By Day 5, the embryo reveals far more: how well it expanded, the quality of the inner cell mass, and the quality of the trophectoderm. This richer picture lets the embryologist choose the single best embryo to transfer with much greater confidence, which is exactly what makes safe single-embryo transfer possible (more on that below).
Day 3 vs Day 5 Transfer — The Honest Success-Rate Comparison
Here is where most articles oversimplify. You will often read “Day 5 has higher success” as a flat statement. The truth is more nuanced — and understanding it will make you a better-informed patient.
| Factor | Day 3 (Cleavage) | Day 5 (Blastocyst) |
|---|---|---|
| Embryo stage | 6–8 cells | ~100+ cells, organised blastocyst |
| Implantation rate per embryo | Lower (often under 20%) | Higher (more advanced + selected) |
| Clinical pregnancy per transfer | Lower in most studies | Higher in most studies |
| Embryo selection confidence | Limited (Day-3 morphology predicts poorly) | Strong (much more information) |
| Risk of no embryo to transfer | Lower — more embryos available Day 3 | Higher — some may not reach Day 5 |
| Enables PGT-A genetic testing | No | Yes (trophectoderm biopsy) |
| Enables safe single-embryo transfer | Harder | Yes — the modern standard |
Per-Transfer vs Per-Retrieval — The Nuance That Matters
Here is the honest version that builds real understanding. Blastocysts have a higher success rate per embryo transferred — that part is well established. But there is a catch: not every fertilised egg survives to become a blastocyst. Only about 30–50% typically reach Day 5. So if you measure success per egg retrieval (the more complete way to think about a whole cycle), the gap between Day 3 and Day 5 can narrow considerably, and in some patients, the live birth rate per retrieval is similar between the two approaches.
What does this mean for you in practice? It means Day-5 transfer is not a magic upgrade that suits everyone identically. It is a powerful tool that helps most strongly when you have enough embryos for the laboratory to apply that natural selection step. When you have very few embryos, transferring earlier at Day 3 can be the safer choice — because waiting risks ending up with no embryo to transfer at all. A good clinic decides this with you, based on your specific situation — not by applying a one-size-fits-all rule.
Understanding Your Embryo Grade — Decoding 4AA, 5AB & 3BB
When your embryos reach the blastocyst stage, the embryologist gives each one a grade using the Gardner grading system — the global standard developed by Dr. David Gardner in 1999. The grade looks like a code: a number followed by two letters, such as 4AA, 5AB, or 3BB. Here is exactly what each part means.
The Number — Expansion (1 to 6)
The first number describes how expanded the blastocyst is — how far along it is in the blastocyst stage:
| Grade | Stage | What It Means |
|---|---|---|
| 1 | Early blastocyst | Fluid cavity is less than half the embryo |
| 2 | Blastocyst | Fluid cavity is half or more of the embryo |
| 3 | Full blastocyst | Fluid cavity fills the embryo completely |
| 4 | Expanded blastocyst | Enlarged, with the outer shell (zona) thinning |
| 5 | Hatching blastocyst | Beginning to break out of its shell |
| 6 | Hatched blastocyst | Fully escaped from the shell, ready to implant |
The First Letter — Inner Cell Mass (A to C)
The inner cell mass (ICM) is the cluster of cells that will become your baby — arguably the most important part. It is graded:
- A: Tightly packed, many cells (best)
- B: Loosely grouped, several cells
- C: Very few cells
The Second Letter — Trophectoderm (A to C)
The trophectoderm (TE) is the outer layer of cells that will form the placenta. It is graded the same way:
- A: Many cells forming a cohesive layer (best)
- B: Few cells forming a loose layer
- C: Very few, large cells
Day 5 vs Day 6 Blastocyst — Does the Day Matter?
Sometimes an embryo does not reach the blastocyst stage until Day 6 instead of Day 5. Patients often worry this means a “weaker” embryo. The honest answer: a Day-6 blastocyst is still very much viable and produces many healthy pregnancies. Research does suggest that, on average, Day-5 blastocysts have somewhat higher pregnancy rates than Day-6 blastocysts — particularly in women under 35 — likely because reaching blastocyst a little faster is a marker of embryo strength. But a good-quality Day-6 blastocyst is far better than no blastocyst, and for many patients it is exactly the embryo that becomes their baby. Day 6 is a slight timing difference, not a failure.
Who Should — and Who Shouldn’t — Choose Blastocyst Transfer
This is the section most articles skip, and it is the most important one for making a good decision. Blastocyst transfer is excellent for many patients — but not the automatic right answer for everyone.
| Situation | Blastocyst (Day 5) Often Suitable? |
|---|---|
| Good number of fertilised embryos available | Yes — ideal. The lab can select the strongest blastocyst. |
| Younger patient with good egg quality | Yes — strong candidate, high blastocyst formation likely |
| Planning PGT-A genetic testing | Yes — blastocyst stage is required for biopsy |
| Wanting single embryo transfer (avoid twins) | Yes — Day 5 makes safe eSET possible |
| Previous IVF failure with Day-3 transfers | Often yes — extended culture reveals embryo development |
| Very few embryos (1–2 fertilised) | Sometimes Day 3 is safer — avoids risk of no embryo reaching Day 5 |
| Older patient with low embryo numbers | Individualised — your specialist weighs the trade-off with you |
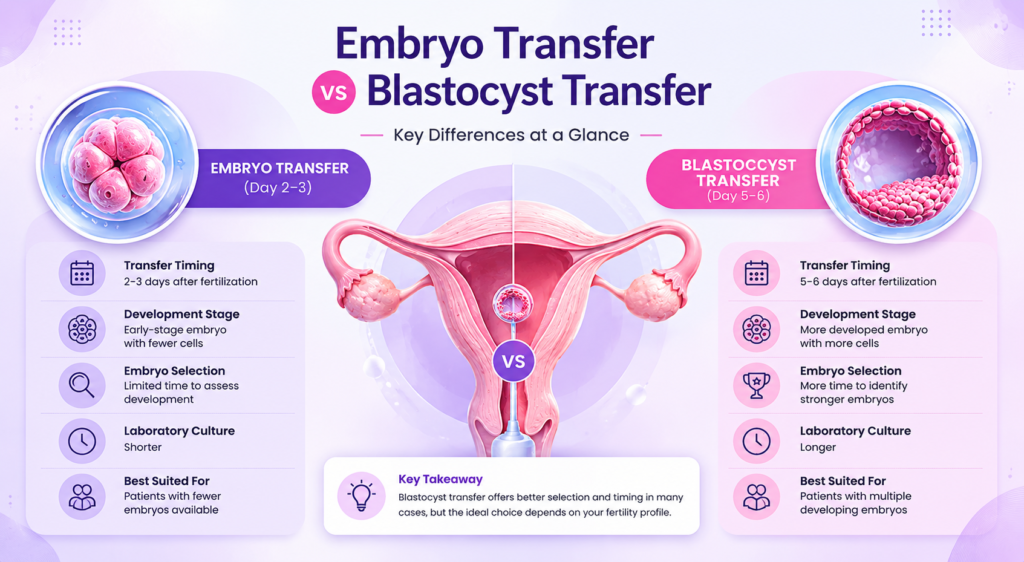
Embryo Transfer vs Blastocyst Transfer: Which Is Better?
Many people assume embryo transfer and blastocyst transfer are different procedures, but a blastocyst is actually a later stage of embryo development. The main difference is when the embryo is transferred into the uterus after fertilisation.
In a standard embryo transfer, embryos are usually transferred on Day 2–3, while blastocyst transfer happens on Day 5–6. Blastocyst transfer allows fertility specialists more time to observe embryo growth and select embryos with stronger developmental potential. However, there is no one-size-fits-all approach.
Blastocyst transfer can help specialists identify embryos with stronger developmental potential, but it is not automatically the best choice for every patient. The ideal option depends on age, embryo quality, ovarian reserve, previous IVF history, and the number of embryos available.
| Factor | Embryo Transfer (Day 2–3) | Blastocyst Transfer (Day 5–6) |
|---|---|---|
| Development Stage | Early-stage embryo with fewer cells | More developed embryo with more cells |
| Transfer Timing | 2–3 days after fertilization | 5–6 days after fertilization |
| Embryo Selection | Limited time for assessment | More time to select stronger embryos |
| Implantation Potential | Good depending on individual factors | Often improved in selected cases |
| Suitable For | Patients with fewer embryos available | Patients with multiple developing embryos |
| Risk of No Transfer | Lower | Slightly higher if embryos stop growing |
| Laboratory Culture Time | Shorter | Longer |
The question is usually not “Which is better?” but rather “Which option is better for your fertility profile?” The ideal choice is the one that offers the highest chance of a healthy pregnancy for an individual patient.
Blastocyst Transfer, PGT-A & Single Embryo Transfer (eSET)
Blastocyst transfer is the foundation of two of the most important advances in modern IVF — both of which improve safety and success:
PGT-A Genetic Testing
Preimplantation Genetic Testing for Aneuploidy (PGT-A) screens an embryo for the correct number of chromosomes before transfer. It is only possible at the blastocyst stage, because the test requires a small biopsy of a few cells from the trophectoderm (the future placenta layer) — leaving the inner cell mass that becomes the baby untouched. Transferring a chromosomally normal (euploid) blastocyst can meaningfully raise implantation rates, especially for older patients or those with recurrent miscarriage.
Elective Single Embryo Transfer (eSET)
Because a Day-5 blastocyst gives the embryologist confidence about which single embryo is strongest, it makes elective single embryo transfer safe and effective. Studies consistently show that transferring one good blastocyst achieves live birth rates similar to transferring two Day-3 embryos, while roughly halving the risk of twins. Twin pregnancies carry significantly higher risks for both mother and babies, so eSET with a blastocyst is increasingly the recommended modern standard for suitable patients in Patna.
Blastocyst Transfer in India — Cost & Lab Capability
An important and rarely-discussed point: blastocyst culture requires an advanced embryology laboratory. Growing embryos reliably to Day 5 needs high-quality culture media, precisely controlled incubators, stable conditions, and skilled embryologists. Not every IVF clinic can do this consistently, which is one reason some clinics still default to Day-3 transfers. When choosing a clinic, it is entirely reasonable to ask: “Does your lab routinely culture embryos to the blastocyst stage?”
On cost: in India, a full IVF cycle that includes blastocyst culture and a single embryo transfer typically ranges from approximately ₹1.2 to ₹1.75 lakh, usually including ovarian stimulation, egg retrieval, fertilisation (often with ICSI), extended culture to the blastocyst stage, the transfer itself, and freezing (vitrification) of any surplus blastocysts for future use. PGT-A genetic testing, if chosen, is an additional cost. A complete itemised estimate should always be provided before treatment begins.
Blastocyst Transfer at Shradha IVF & Maternity in Patna
At Shradha IVF & Maternity, blastocyst culture and transfer are performed routinely in our embryology laboratory, with the approach individualised to each couple:
- Advanced blastocyst-culture lab: our embryology laboratory cultures embryos to the Day-5/6 blastocyst stage as standard practice — Test Tube Baby Centre in Patna
- Individualised transfer-day decisions: Day 3 vs Day 5 is decided with each couple based on embryo number, age, and history — never by a blanket rule
- Single embryo transfer where suitable: to maximise a healthy singleton pregnancy and minimise twin-related risks
- Transparent cost & EMI options: cost of IVF treatment and IVF on EMI
- Direct guidance from Dr. Shradha Chakhaiyar— every transfer plan is reviewed personally
FAQs on Understanding Blastocyst Transfer
Blastocyst transfer generally has good success rates because the embryo has already developed for about 5–6 days before transfer, allowing specialists to select embryos with stronger developmental potential. Success rates can vary widely based on factors such as maternal age, embryo quality, uterine health, and whether genetically tested embryos are used. Younger women and high-quality embryos often have higher implantation and pregnancy rates, but outcomes are always individual.
Around 5 days after a blastocyst transfer, implantation may already be occurring or may have recently completed. The embryo begins attaching to the uterine lining and, if implantation is successful, starts producing the hormone hCG. Most people do not notice symptoms at this stage, while others may experience mild cramping, light spotting, bloating, or no symptoms at all. Symptoms alone cannot reliably confirm pregnancy.
A blastocyst is also an embryo—it is simply a more advanced stage of embryo development. Early embryo transfers usually happen on day 2–3, while blastocyst transfers happen on day 5–6. Blastocyst transfer is often preferred because it allows better selection of embryos with stronger growth potential and may improve implantation chances. However, it is not automatically the best option for everyone. The choice depends on the number of embryos available, embryo development, age, and individual fertility factors.
A 5-day blastocyst usually starts implanting within about 1–3 days after transfer and implantation is often completed within around 2–5 days. Because the embryo has already reached an advanced stage before transfer, implantation tends to occur sooner than with earlier-stage embryo transfers. Pregnancy testing is commonly recommended around 9–14 days after transfer for more reliable results.
The Right Embryo, Transferred at the Right Time.
At Shradha IVF & Maternity in Patna, Dr. Shradha Chakhaiyar and our embryology team decide your transfer day around your specific cycle — using advanced blastocyst culture when it helps, and being honest when it doesn’t.
Book Your Consultation at Shradha IVF →