Reviewed by Dr. Shradha Chakhaiyar, MBBS, DGO, MRCOG (London), IVF Specialist & Reproductive Surgeon
Shradha IVF & Maternity, Patna, Bihar · 20+ Years Clinical Experience
📋 Table of Contents
- The News: PCOS Is Now PMOS
- Why Did the Name Change?
- PCOS vs PMOS — What’s Different?
- Symptoms by Body System
- The Insulin Resistance Connection
- How Is PMOS Diagnosed?
- PMOS in India & “Lean PMOS”
- PMOS and Fertility
- What Should You Do Now?
- PMOS and Mental Health
- Treatment at Shradha IVF, Patna
- Frequently Asked Questions
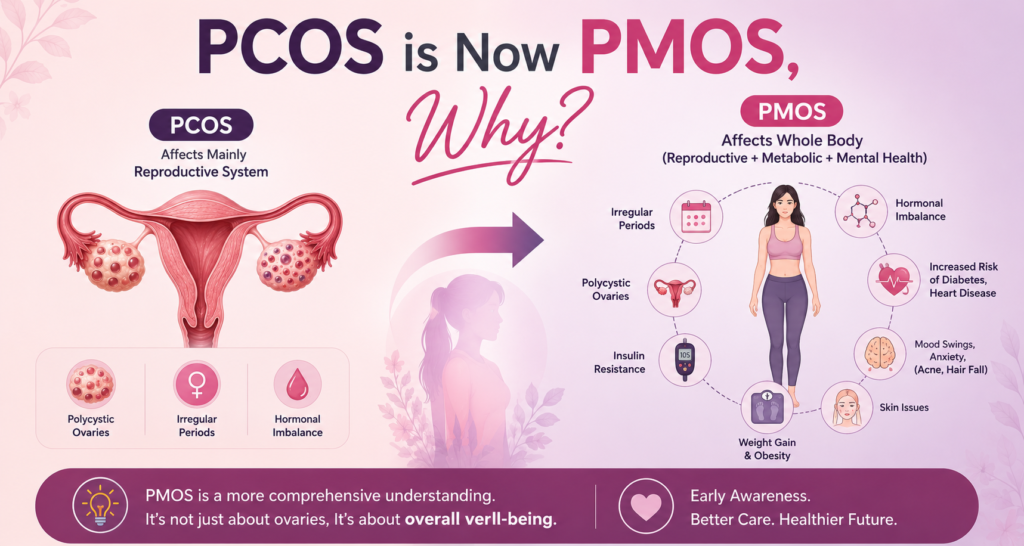
The News: PCOS Has Officially Been Renamed PMOS
PMOS stands for Polyendocrine Metabolic Ovarian Syndrome. It is the new name for the condition previously known as PCOS (Polycystic Ovary Syndrome). The change was announced in a global consensus published in The Lancet on 12 May 2026. The new name reflects that the condition is a whole-body hormonal and metabolic disorder — not just an ovary problem — and that the “cysts” the old name referred to are not actually cysts at all.
On 12 May 2026, a landmark paper was published in The Lancet — one of the world’s most respected medical journals — formally renaming Polycystic Ovary Syndrome (PCOS) to Polyendocrine Metabolic Ovarian Syndrome (PMOS). This was not a single doctor’s opinion or a social-media trend. It was the result of an unprecedented global consensus process led by Professor Helena Teede of Monash University in Australia, involving more than 56 leading academic, clinical, and patient organisations across 71 countries.
The decision was grounded in the largest patient-engagement effort ever undertaken for a health-condition name change: more than 14,000 survey responses from women with the condition and from healthcare professionals (and over 22,000 voices across the full 11-year process). When the new name was put to a vote, 85.6% of patients and 76.1% of health professionals supported the change. The condition affects roughly 1 in 8 women — more than 170 million worldwide — making this one of the most significant women’s health developments of the decade.
A three-year transition period is now underway, supported by an international education campaign and updates to clinical guidelines, medical education, and international disease-classification systems. In other words: the change is official, it is permanent, and over the next few years you will see “PMOS” gradually replace “PCOS” in clinics, reports, and guidelines around the world.

Why Did the PCOS Name Changed to PMOS? — The Problem With “Polycystic”
For decades, both doctors and patients have known that “Polycystic Ovary Syndrome” was a misleading name. Here is the core problem: the “cysts” the name refers to are not actually cysts at all.
What appears as small dark circles on an ovarian ultrasound in this condition are not pathological cysts — they are arrested follicles, small immature egg sacs that have not matured and released an egg. They are a normal part of how the ovary works, just present in greater numbers and not progressing as they should. In fact, a related paper published alongside the consensus confirmed there is no increase in abnormal ovarian cysts in women with the condition. The name was describing something that was never really there.
This misnaming caused real harm. Because the name pointed at the ovaries and at “cysts,” it led to three damaging misunderstandings:
- Women believed they only had an ovarian problem — when the condition actually affects insulin, metabolism, multiple hormones, skin, mood, and long-term heart and metabolic health.
- Diagnosis was delayed — research shows up to 70% of those with the condition experienced diagnostic delays, partly because doctors looking for “cysts” did not find the textbook picture.
- Care was fragmented — the condition was treated as a narrow gynaecological issue rather than the whole-body metabolic disorder it is.
The new name fixes each piece. Polyendocrine acknowledges the multiple hormones involved (insulin, androgens, neuroendocrine hormones). Metabolic recognises the central role of insulin resistance and the raised risks of diabetes and heart disease. Ovarian keeps the link to ovarian function and fertility, which remains real. Together: Polyendocrine Metabolic Ovarian Syndrome.
PCOS vs PMOS — What’s Actually Different?
If you have PCOS, here is the most important reassurance: you do not have a new or different disease. PMOS is the same condition you have always had. What has changed is the name and, with it, the medical understanding of where the real problem lies. Here is the side-by-side:
| Aspect | Old: PCOS | New: PMOS |
|---|---|---|
| Full name | Polycystic Ovary Syndrome | Polyendocrine Metabolic Ovarian Syndrome |
| What it emphasises | The ovaries and “cysts” | Whole-body hormones + metabolism + ovaries |
| The “cysts” | Implied pathological cysts | Recognised as arrested follicles, not true cysts |
| Core driver highlighted | Ovarian dysfunction | Insulin resistance & hormonal imbalance |
| The condition itself | Same condition | Same condition — only the name & framing changed |
| Your diagnosis | Still valid | Still valid — no need to be re-diagnosed |
| Treatment | Still effective | Same treatments, now applied more whole-body |
PMOS Is a Whole-Body Condition — Symptoms by System
The reason the name change matters is captured in this list. PMOS does not stay in the ovaries. Its symptoms appear across multiple body systems — which is exactly why so many women spent years being told their separate symptoms were unrelated:
| Body System | Common PMOS Symptoms |
|---|---|
| Reproductive | Irregular or absent periods, difficulty conceiving, irregular ovulation, heavy or unpredictable bleeding |
| Metabolic | Weight gain (especially around the abdomen), difficulty losing weight, insulin resistance, sugar cravings, fatigue after meals |
| Skin & Hair | Acne, oily skin, excess facial/body hair (hirsutism), scalp hair thinning, dark velvety skin patches (acanthosis nigricans) on neck and underarms |
| Mental & Emotional | Anxiety, low mood, body-image distress, reduced confidence, emotional exhaustion from fertility struggles |
| Long-term Risk | Higher risk of type 2 diabetes, fatty liver, high blood pressure, high cholesterol, and cardiovascular disease |
If you recognise yourself in symptoms across several of these rows — not just the reproductive one — that is the whole point of the new name. These are not separate problems. They are one connected condition.
The Insulin Resistance Connection — The Engine Behind PMOS
If there is one concept to take away from the PMOS reframe, it is this: insulin resistance is often the engine driving the whole condition.
Insulin is the hormone that moves sugar from your blood into your cells. In insulin resistance, your cells respond poorly to insulin, so your body produces more and more of it to compensate. Those high insulin levels then do something specific in the ovaries: they stimulate the ovaries to produce more male hormones (androgens). Excess androgens disrupt ovulation, drive acne and excess hair growth, and worsen the whole picture. High insulin also makes weight gain easier and weight loss harder — which feeds back into more insulin resistance. It is a self-sustaining cycle.
This is why modern treatment increasingly targets insulin and metabolism — through nutrition, movement, and where appropriate, insulin-sensitising support like inositol or metformin — rather than focusing only on the ovaries or only on regulating periods. Fix the engine, and many of the downstream symptoms improve together.
How Is PMOS Diagnosed? — The Rotterdam Criteria & the 4 Types
Despite the name change, the way the condition is diagnosed has not changed. Doctors still use the internationally endorsed Rotterdam criteria, which require at least two of the following three features to be present (after excluding other conditions):
- Ovulatory or menstrual dysfunction — irregular, infrequent, or absent periods
- Hyperandrogenism — excess male hormones, shown either by a blood test or by physical signs like excess facial/body hair, acne, or scalp hair loss
- Polycystic ovarian morphology on ultrasound — many small follicles (the “arrested follicles”) or enlarged ovaries. Note: if you have the first two features, an ultrasound is not even needed to diagnose.
Because you only need two of three, the condition shows up in four different patterns, called phenotypes:
| Type | Features Present | What It Tends to Mean |
|---|---|---|
| Phenotype A | All three (androgens + irregular ovulation + ovary morphology) | The most complete and often most metabolically significant form |
| Phenotype B | High androgens + irregular ovulation | Strong metabolic and hormonal involvement |
| Phenotype C | High androgens + ovary morphology | “Ovulatory” form — periods may be regular |
| Phenotype D | Irregular ovulation + ovary morphology (no excess androgens) | The mildest metabolic picture; sometimes mainly ovarian |
Knowing your phenotype matters because treatment is not one-size-fits-all. A woman with Phenotype A and significant insulin resistance needs a different plan than a woman with Phenotype D and regular cycles. This is exactly the personalised, whole-body thinking the PMOS name is meant to encourage.
PMOS in India — Why It’s More Common Here, and “Lean PMOS”
PMOS is not a rare condition in India — it is extremely common, and arguably more common here than in much of the world. While the global prevalence is around 1 in 8 women, Indian studies using the Rotterdam criteria report a pooled prevalence of roughly 10–11%, and some regional studies suggest as many as 1 in 5 young Indian women are affected. Several factors contribute: genetic predisposition in South Asian populations toward insulin resistance, rapid dietary and lifestyle changes, and rising rates of metabolic disease.
Indian women are also disproportionately affected by “lean PMOS” — having the condition at a normal body weight. South Asians tend to carry more visceral (internal) fat and have higher insulin resistance at any given body weight than many other populations. This means a slim Indian woman can have significant insulin resistance and full PMOS while being repeatedly told she “looks fine” and dismissed. If that has been your experience, it does not mean you are imagining your symptoms. It means you need proper testing — including direct insulin and metabolic assessment — not just a glance at the weighing scale.
PMOS and Fertility — Can You Still Get Pregnant?
Yes. The vast majority of women with PMOS can get pregnant — many naturally, and most of the rest with treatment. PMOS is one of the most treatable causes of infertility. In fact, women with PMOS often have an advantage in fertility treatment: they tend to be younger at diagnosis and usually have a high ovarian reserve (high AMH and plenty of eggs). The challenge is not a shortage of eggs — it is getting those eggs to ovulate reliably.
Here is how fertility treatment typically progresses, from least to most intensive:
1. Lifestyle and Weight — The Powerful First Step
For women who are overweight, even a 5–10% reduction in body weight can restore regular ovulation and dramatically improve natural conception chances. A balanced, lower-glycaemic diet, regular movement, good sleep, and stress management all directly improve insulin sensitivity. This is genuinely first-line treatment — not a throwaway “just lose weight,” but a targeted metabolic intervention.
2. Inositol and Metformin — Targeting Insulin
Myo-inositol (often combined with D-chiro-inositol) is a well-tolerated supplement that can improve insulin sensitivity and ovulation in many women with PMOS, with limited risk. Metformin, a diabetes medication used off-label, can improve insulin resistance and menstrual regularity — it is particularly considered in women with prediabetes or significant insulin resistance. Your doctor will advise which, if either, suits your phenotype.
3. Ovulation Induction — Letrozole and Clomiphene
If lifestyle changes alone do not restore ovulation, ovulation-induction medicines are the next step. Letrozole is now generally preferred over clomiphene as first-line for PMOS ovulation induction, as evidence shows higher live-birth rates in many women. These are typically combined with cycle monitoring to confirm ovulation and time of conception.
4. IUI (Intrauterine Insemination)
If ovulation induction alone is not enough, or if there are additional mild factors, IUI with mild stimulation adds a step by placing prepared sperm directly into the uterus around ovulation — improving the odds per cycle while remaining far less intensive than IVF.
5. IVF — and an Important Safety Point
When other treatments do not succeed, IVF treatment in Patna is highly effective for PMOS, with success rates of roughly 40–50% per cycle for women under 35, often comparable to or better than other causes of infertility, precisely because of the good egg numbers. But there is a crucial safety point: women with PMOS have a higher risk of Ovarian Hyperstimulation Syndrome (OHSS), because their ovaries respond strongly to stimulation. A skilled clinic manages this with gentler stimulation protocols, careful monitoring, and frequently a “freeze-all” approach — freezing the embryos and transferring them in a later, safer cycle. Choosing an experienced fertility specialist is not optional for PMOS patients; it is what keeps IVF both effective and safe.
What Should You Do Now? — Practical Guidance
If you have PMOS (or PCOS — same thing), here is exactly what the name change means for your next steps:
- Do not panic and do not get re-diagnosed. Your diagnosis is unchanged and still valid.
- Do not stop treatment that is working. Existing treatments remain effective.
- Do use this as a prompt to check your metabolic health. Ask your doctor about fasting insulin, fasting glucose or HbA1c, a lipid profile, and vitamin D — not just a hormone panel. The whole-body framing of PMOS is the actionable part.
- If you have been dismissed because you are slim, seek proper insulin testing. Lean PMOS is real and common in India.
- If you are trying to conceive, get evaluated sooner rather than later. PMOS is highly treatable, and early, personalised care produces the best outcomes.
PMOS and Mental Health — The Part No One Talks About
One of the quiet strengths of the PMOS reframe is that it formally recognises the psychological dimension of the condition. Women with PMOS experience higher rates of anxiety, depression, and body-image distress — driven partly by the hormonal and metabolic changes themselves, and partly by years of confusing symptoms, weight struggles, dismissive consultations, and, for many, the emotional weight of infertility.
This is not a side issue. Emotional health affects sleep, stress hormones, eating patterns, and treatment adherence — all of which feed back into the metabolic picture. Modern PMOS care treats mental well-being as part of the treatment, not an afterthought. If you have been carrying this silently, please know: your symptoms are real, your frustration is valid, and the condition is treatable.
How Shradha IVF Treats PMOS-Related Infertility in Patna
At Shradha IVF & Maternity, PMOS-related infertility is evaluated and treated with the whole-body approach the new name calls for:
- Complete metabolic + hormonal evaluation: not just hormones, but insulin, glucose, thyroid, vitamin D, and lipid assessment to find the real driver
- Phenotype-based personalised treatment: matching the plan to your specific PMOS type rather than a generic protocol
- OHSS-safe IVF protocols: gentle stimulation, close monitoring, and freeze-all strategies where appropriate — best fertility specialist in Patna
- Transparent cost & EMI options: cost of IVF treatment and IVF on EMI
- Free pre-treatment consultation available at our regular IVF Camp
FAQs Related to PMOS
PMOS (Polyfollicular Morphological Ovary Syndrome) is a newer way of looking at the condition beyond only ovarian cyst appearance. Unlike PCOS, PMOS considers the whole-body effects, including hormones, metabolism, ovulation, and fertility.
The term PMOS is being discussed because many experts believe PCOS does not fully describe the condition. The syndrome affects multiple body systems, not just the ovaries.
Yes. PMOS can affect ovulation and menstrual cycles, which may make it harder to conceive naturally in some women. However, many women with PMOS can achieve pregnancy with proper treatment and lifestyle management.
Yes. Many women with PMOS conceive naturally, especially when ovulation is regular or after improving lifestyle factors and hormone balance.
PMOS diagnosis may involve medical history, symptom evaluation, hormone blood tests, ultrasound scans, and assessment of ovulation patterns.
PMOS Is Treatable — and Pregnancy Is Possible.
The name has changed, but the message for you is hopeful: PMOS is one of the most treatable causes of infertility. At Shradha IVF in Patna, Dr. Shradha Chakhaiyar builds a whole-body, personalised plan around your specific PMOS type — not a generic protocol.
Book Your Free Consultation →