
Medically Reviewed by Dr. Shradha Chakhaiyar, MBBS, DGO, MRCOG (London) — Fertility Specialist & Reproductive Surgeon, Shradha IVF & Maternity, Patna
20+ Years of Experience · www.shradhaivf.com
Most fibroids do not cause infertility — their location matters most. Submucosal fibroids (inside the uterine cavity) most often affect fertility by blocking implantation, and usually should be removed. Subserosal fibroids (on the outer wall) generally do not affect fertility. Intramural fibroids (in the muscle wall) may matter if large or distorting the cavity. Many women with fibroids conceive naturally.
📋 What This Guide Covers
- What are uterine fibroids?
- How common are they?
- The three types — and why location decides
- How fibroids cause infertility
- Symptoms to watch for
- Can you get pregnant with fibroids?
- Fibroids during pregnancy — the risks
- How fibroids are diagnosed
- Treatment & myomectomy options
- Do fibroids need to be removed?
- Fibroids and IVF
- A note from Dr. Shradha
- FAQs
What Are Uterine Fibroids?
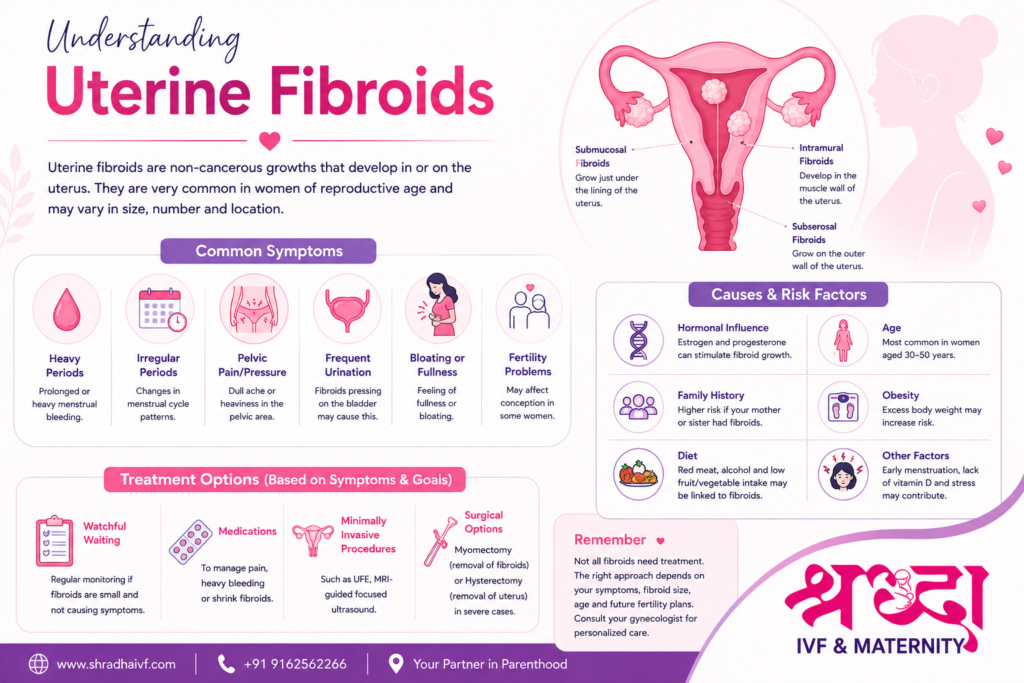
Uterine fibroids — also called leiomyomas or myomas — are non-cancerous growths of muscle and fibrous tissue that develop in or on the uterus. They are the most common benign tumour in women, and they do not raise your risk of cancer. They can be as small as a pea or as large as a melon, single or multiple, and they grow under the influence of the hormones oestrogen and progesterone — which is why they often appear during the reproductive years and tend to shrink after menopause.
The crucial point for fertility is not that you have a fibroid, but what kind and where it is.
How Common Are Fibroids?
Very common — and this context matters, because it should reduce your alarm. By the age of 50, somewhere between 20% and 80% of women will have developed fibroids. Yet only about 5–10% of women with infertility have fibroids at all, and fibroids are the sole cause of infertility in just 2–3% of cases. In other words, most women with fibroids are fertile, and most fibroids are silent bystanders rather than the cause of a problem. The job of a good evaluation is to work out whether your particular fibroid is one of the few that actually matters.
The Three Types of Fibroid — and Why Location Decides Everything
Fibroids are classified by where they grow, and this classification is the single most important thing to understand, because it predicts whether fertility is affected:
| Type | Where it grows | Effect on fertility | Remove for fertility? |
|---|---|---|---|
| Submucosal | Bulges into the uterine cavity (under the lining) | Highest impact — blocks implantation, acts like an IUD, raises miscarriage risk | Usually yes |
| Intramural | Within the muscular wall of the uterus | Depends — matters if large (roughly >4–5 cm) or distorting the cavity | Sometimes — individualised |
| Subserosal | On the outer wall, projecting outward | Usually none — rarely affects fertility | Usually no |
This is the reframe that changes everything: a large subserosal fibroid on the outside of your uterus may look dramatic on a scan but leave your fertility untouched, while a small submucosal fibroid inside the cavity — easy to overlook — can be the real obstacle. Size matters, but location matters more.
How Fibroids Cause Infertility (When They Do)
When a fibroid does interfere with fertility, it usually does so through one or more of these mechanisms:
- Distorting the uterine cavity — a submucosal fibroid deforms the surface where the embryo needs to implant, physically preventing attachment.
- Blocking the fallopian tubes — a fibroid near the tubal openings can stop the egg and sperm from meeting.
- Changing the cervix — a fibroid near the cervix can alter its shape and reduce the number of sperm that enter.
- Impairing blood flow to the lining — reducing the endometrium’s ability to support an implanting embryo.
- Increasing uterine contractions (peristalsis) — intramural fibroids can disturb the gentle wave-like movements of the uterus, interfering with implantation.
- Causing inflammation — altering the local environment and the lining’s receptivity.
You’ll notice these all come back to the same theme: it’s fibroids that reach or distort the cavity that cause trouble, which is exactly why location is the deciding factor. (For more on why a healthy lining matters so much, see our guide on the importance of the uterine lining in IVF.)
What are the Symptoms of Fibroids to Watch For?
Many fibroids cause no symptoms at all and are found incidentally on a scan. When symptoms do occur, they may include:
- Heavy or prolonged menstrual bleeding (a very common sign)
- Periods lasting more than seven days
- Pelvic pain, pressure, or a feeling of fullness
- Frequent urination or difficulty emptying the bladder
- Constipation or bowel pressure
- Lower back pain
- Pain during intercourse
- Fatigue and anaemia from heavy blood loss
- Difficulty conceiving or recurrent miscarriage
Heavy periods deserve special mention. In Bihar, heavy menstrual bleeding is often tolerated for years as “normal,” which delays diagnosis and worsens anaemia. It is not something you have to simply live with — it’s worth investigating. If your periods are heavy or your uterus has been called bulky on a scan, a proper evaluation is wise.
Can You Get Pregnant With Fibroids?
Yes — in the great majority of cases, you can. Most women with fibroids conceive naturally without any treatment, particularly when the fibroids are small, subserosal, or intramural without cavity distortion. Fibroids do not affect ovulation, so your eggs and cycles are usually unaffected. Where fibroids do reduce fertility — most often submucosal ones — treatment is usually straightforward and restores good pregnancy odds. So a fibroid diagnosis is rarely a barrier to motherhood; it’s simply something to assess and, if needed, address.
Fibroids During Pregnancy — The Honest Risks
Most women with fibroids have completely normal pregnancies. But it’s fair to be honest that fibroids — particularly larger ones — can occasionally raise the risk of certain complications, so they’re worth monitoring:
- Slightly higher risk of miscarriage, especially with submucosal fibroids
- Red degeneration — a fibroid outgrowing its blood supply in pregnancy, causing pain (usually managed with rest and pain relief)
- Preterm labour or placental problems with large fibroids
- Fetal malposition (e.g. breech), sometimes making a caesarean more likely
These are possibilities, not certainties — and with good antenatal monitoring, the outcomes are usually excellent. The point is not to worry, but to be followed by a specialist who knows your fibroids are there.
How Fibroids Are Diagnosed?
The goal of diagnosis is not just to find a fibroid, but to map its exact type, size, and — crucially — its relationship to the cavity. The tools:
- Pelvic / transvaginal ultrasound — the first-line test; detects fibroids and gives size and rough location.
- Saline sonohysterography (SIS) — saline is instilled into the cavity during ultrasound to reveal whether a fibroid is distorting it (very useful for spotting submucosal fibroids).
- Hysteroscopy — a thin camera passed through the cervix to directly view the cavity; the gold standard for confirming and often treating submucosal fibroids.
- MRI — for precise mapping when fibroids are large, multiple, or when surgery is being planned.
Treatment & Myomectomy Options for Treating Uterine Fibroids
Treatment is guided by one question above all: is this fibroid actually affecting your fertility or causing significant symptoms? If not, the best treatment is often none at all. When treatment is warranted, the options range from watching to medication to uterus-preserving surgery.
Watchful waiting
For small, asymptomatic fibroids — especially subserosal ones — regular monitoring with follow-up scans is often all that’s needed.
Medication
Medications (hormonal treatments, GnRH agonists to temporarily shrink fibroids before surgery, tranexamic acid for heavy bleeding) can control symptoms. Important caveat: most hormonal treatments are not compatible with actively trying to conceive, so they’re used to manage symptoms or prepare for surgery, not as a fertility treatment in themselves.
Myomectomy — surgical removal that preserves the uterus
For fibroids affecting fertility, myomectomy — removing the fibroid while keeping the uterus intact — is the fertility-preserving procedure of choice (very different from hysterectomy, which removes the uterus). There are three approaches, matched to the fibroid:
| Approach | Best for | Try to conceive after |
|---|---|---|
| Hysteroscopic myomectomy | Submucosal fibroids (through the cervix, no incision) | Often the next cycle after healing |
| Laparoscopic myomectomy | Intramural / subserosal fibroids (keyhole surgery) | Usually after ~3 months of healing |
| Open (abdominal) myomectomy | Large or multiple fibroids | After ~3 months; C-section advised for future deliveries |
One option to avoid if you want to conceive: uterine artery embolisation (UAE). While effective for symptom control, it can compromise blood supply to the uterus and is generally not recommended for women who still wish to become pregnant. Myomectomy is preferred in that situation.
Do Fibroids Need to Be Removed Before Pregnancy?
Not always — and this is where an experienced specialist matters, because over-treatment is a real risk. A reasonable framework:
- Submucosal fibroids distorting the cavity → removal is usually recommended, as it improves pregnancy rates.
- Intramural fibroids → individualised; removal is considered when they’re large or distorting the cavity, or when there’s unexplained infertility or recurrent miscarriage. Small, non-distorting ones are often left alone.
- Subserosal fibroids → removal for fertility is generally not needed.
The decision always balances the fibroid’s effect against the fact that surgery itself has recovery time and risks. A good fertility surgeon removes what needs removing — and, just as importantly, leaves alone what doesn’t.
Fibroids and IVF
If you’re planning IVF, the same principle applies. Submucosal fibroids are usually removed before an IVF cycle, because they reduce implantation rates. Cavity-distorting intramural fibroids are often addressed, too. Subserosal and small non-distorting intramural fibroids usually don’t need treatment before IVF. At Shradha IVF, we assess each fibroid’s relationship to the cavity precisely, so your IVF cycle starts with the best possible uterine environment — and we don’t operate unnecessarily.
A Note from Dr. Shradha, Patna
At Shradha IVF & Maternity, fibroid evaluation and uterus-preserving myomectomy are performed under the personal care of Dr. Shradha Chakhaiyar, MRCOG (London), with advanced hysteroscopic and laparoscopic capability in Patna — so you don’t need to travel to a metro for expert care. The first consultation is free.
Worried a Fibroid Is Affecting Your Fertility?
Most fibroids don’t — but the only way to know is a proper evaluation of where yours sits. Dr. Shradha will assess it precisely and give you an honest plan: reassurance, monitoring, or uterus-preserving surgery only if truly needed. The first consultation is free.
FAQs Related to Uterine Fibroids
Fibroids usually develop in the uterus, not the ovaries. Their seriousness depends on size, location, and symptoms. Some are harmless, while others may cause heavy bleeding, pain, pressure, or fertility problems. Large or rapidly growing fibroids should be evaluated by a gynecologist for proper treatment planning.
Fibroids are generally uterine growths, but symptoms linked to pelvic masses may include lower abdominal pain, bloating, heavy or painful periods, frequent urination, pelvic pressure, pain during intercourse, or difficulty conceiving. Sometimes small fibroids cause no symptoms and are found during routine ultrasound scans.
Treatment depends on the size, symptoms, age, and fertility goals. Options may include medicines to control symptoms, hormonal therapy, minimally invasive procedures, or surgery such as myomectomy. Doctors recommend treatment only when fibroids cause pain, heavy bleeding, fertility issues, or significant discomfort.
Untreated fibroids may continue growing and can cause heavy bleeding, anemia, pelvic pain, pressure symptoms, or fertility complications. Fibroids larger than 5–10 cm or those affecting the uterine cavity may need closer monitoring or treatment, especially if they cause symptoms or pregnancy-related concerns.
No. Most fibroids do not cause infertility — they are the sole cause in only about 2–3% of cases. Whether a fibroid affects fertility depends mainly on its location. Submucosal fibroids inside the cavity are most likely to interfere; subserosal fibroids on the outer wall usually don't affect fertility at all.
Yes, in most cases. Fibroids don't affect ovulation, and many women with fibroids conceive naturally, especially with small, subserosal, or non-cavity-distorting fibroids. Where fibroids do reduce fertility — usually submucosal ones — treatment is generally straightforward and restores good pregnancy chances.
Submucosal fibroids, which grow into the uterine cavity, affect fertility most — they can block embryo implantation and increase miscarriage risk. Intramural fibroids may affect fertility if large or distorting the cavity. Subserosal fibroids, on the outer uterine wall, generally do not affect fertility.